A 47 year old presented with C/O Slurred speech, double vision with both eyes and diminision of vision in the right eye, dizziness when standing or walking, numbness of tongue
This is an a online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
Case:
A 47 year old female homemaker by occupation came to the opd with C/O Slurred speech, double vision with both eyes and diminision of vision in the right eye, dizziness when standing or walking, numbness of tongue since 20-11-2021 10:30am.
HOPI:
Patient was apparently asymptomatic 15 days back then she fell on a bucket as she slipped on a wet floor and got injured lateral to left hypochondriac region, she was experiencing severe pain. The next day she went to an RMP doctor and received two pain killer injections, but the pain did not relieve so she went to an MBBS doctor at Chanduru where he did a scan and said that there is no involvement of bone and the pain was due to involvement of muscle and gave her a pain killer injection, few minutes later she developed-
Slurring of speech which was sudden in onset, developed 1 day back, the speech is not fluent and there is change in voice .
Double vision which was sudden in onset,since 1 day and present when seen with both the eyes, but when seen with either eye closed there is no double vision .
Diminision of vision- in the right eye which was sudden in onset, since 1 day.
Dizziness when the patient is standing or walking, which is sudden in onset since 1day and feels that the patient herself is moving, because of which she's unable to walk without support.
Numbness of tongue which was sudden in onset since 1 day.
No h/o seizures, headache, vomiting, diarrhoea, no difficulty in deglutition.


Past history:
There were no similar complaints in the past.
She's k/c/o DM for past 6years on OHA's(Metformin+Glimiperide).
And K/c/o HTN for past 10 year for which she's on Amlodipine.
Not a k/c/o TB, Asthma, epilepsy, CAD.
Surgical history:
she underwent hysterectomy.
Personal history:
Diet: Mixed
Appetite:Normal
Sleep:Adequate
Bowel and bladder:Regular
Addictions: Nothing.
General examination:
Patient is conscious,coherant, cooperative
She is well oriented to time, place and person.
Moderately built and nourished.
No pallor, icterus, cyanosis, clubbing, lymphadenopathy, edema.
Vitals:
Temperature:afebrile
PR:77bpm
BP:130/80mmhg
RR:19/min
PO2:99%
GRBS: 229mg/dl
Systemic examination:
CNS:
Oriented to time,place,person
Memory : recent, remote intact
Speech: slurred, no dysarthria.
Cranial nerves:
1-intact
2-diplopia in binocular vision
- monocular vision:normal
- colour vision:normal
3,4,6- normal(no restriction of movements of eye)
5-normal( muscles of mastication+sensations of face)
7-normal
8- didn't elicit
9,10,11,12-normal
Motor- tone -normal
Power 4-/5 in b/l lowerlimbs 5/5 in upper limbs
Reflexes :
- biceps:b/l:2+
- triceps:2+
- supinator+
- knee:2+
- plantars:b/l flexor
sensory: crude ,pain,temp, fine touch, joint position, proprioception are normal in all dermatomes
not able to perform rhomberg's (as shes swaying even with eyes open).
Cerebellum-
no finger nose/finger finger incordination
no rebound, dysdiadokinesia.
nystagmus present- gaze evoked , horizontal more on right gaze with fast component towards the right, and seen with upward gaze- vertical upbeat and downbeat +.
Gait: slow paced, swaying on both sides.
Stride:regular with path deviation
turns: normal.
CVS: S1 S2+ no murmurs heard.
Respiratory system- Bilateral air entry+ ,normal vesicular breath sounds-heard
P/A: Soft, non tender, no distension, aumbilicus central and inverted,no scars, no sinuses, hernial orifices free.
Provisional diagnosis:
Lesion at the level of pons and cerebellum.
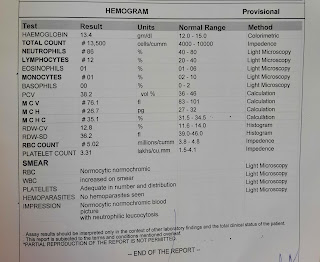
Investigations:


Tab. ECOSPRIN 150mg PO/OD
Tab. CLOPIDOGREL 150mg PO/OD
Inj. NPH S/C BD 20U
Inj. HAI 10U-10U-8U
Tab. BPLEX FORTE OD
Comments
Post a Comment